

Microcephalic primordial dwarfism (MOPD2) is a genetic condition characterized by small stature (microcephalic ophthalmolysis) with other skeletal irregularities (ostelegy). It is characterized by an abnormality in cranial asymmetry and facial development. Some of the most striking characteristics are the presence of a small forehead, flat nose, large cheekbones, broad foreheads, a small chin and a small and long mouth. MOPD2 is found to be inherited from both parents, though it can also develop spontaneously.
The exact causes of MOPD2 are unknown, though it is believed that some combination of genetic and environmental factors may play a role. The exact cause has not been determined, but many experts do agree that it is caused by a deficiency of a gene called ARHGAP2. This gene encodes a protein that is essential for proper brain development.
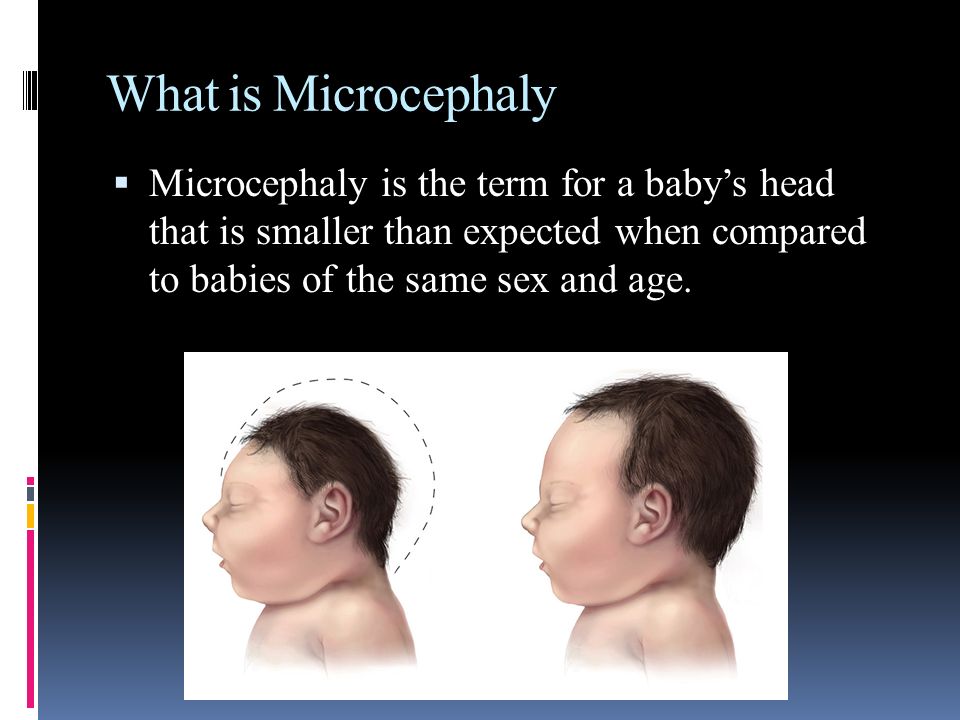
Microcephaly is an umbrella term that refers to a variety of structural defects of the head, including microcephalus, microcephaly or macrocephaly. Microcephaly is the largest cranial abnormality, affecting approximately 40% of the newborns. It is a relatively common disorder affecting all races, ethnicity, and ethnic groups. It occurs mostly in boys, though there are occasional cases of females developing it. It is more commonly seen among African American males than in other racial groups.
MOPD2 can occur due to a variety of reasons. One of them is when a baby is born with abnormally low birth weight. Other causes include exposure to toxins, tumors, infections and other disorders of the central nervous system, congenital adrenal hyperplasia and polycystic ovarian syndrome.
Treatment for MOPD2 can range from routine screening to surgical intervention in rare instances. In the absence of other causes, such treatment usually involves surgery to correct cranial asymmetry and/or replacement of missing bones.
MOPD2 is not commonly detected until adulthood because of the limited visual acuity and poor vision of patients with microcephaly. Because of this, surgical intervention is often the only effective treatment option, although this does not resolve all of the symptoms of the disease. It is possible to improve vision and increase head size through the use of surgical techniques called stereoscopic techniques, such as coronal laser iridotomy, scalpel resurfacing, and coronal rhizotomy.
Other surgical interventions used to treat the symptoms include implantation of extra bone, scalp reduction, adhesions removals, microsurgery, and traction procedures
In some instances, a combination of one or more surgical interventions is used. These procedures are usually combined in conjunction with a comprehensive physical therapy plan.
MOPD2 is not a life-threatening condition. However, its complications can be more severe if it is left untreated for too long.
Minor Cranial Deformities (microcephaly) occur due to different reasons. For example, congenital adrenal hyperplasia (CAH), which occurs due to genetic abnormalities in the adrenal glands of newborns, results in growth of unusually small bones. This type of growth is called microcephaly. Another cause of microcephaly is primary congenital adrenal hyperplasia, or PCAH, a condition where a woman is born with an abnormally small adrenal gland that produces excessive hormones.
The most common type of facial bones involved in this condition is the mandible, which are usually very long and narrow, and rounded, rather than being blunt and flat. The lower jawbone is usually longer than that of the skull, causing the jawbone to recede. At times, it may also appear as an open bite.
Another cause of microcephaly that is not related to hormonal or genetic abnormalities is cleft palate, which occurs as a result of birth defects in the nose or mouth. It is usually caused by the development of a cleft palate on the left side of the child. A cleft palate may also be a result of an abnormality in the opening of the mouth.
Sometimes, the upper jaw bone on one side of the child may be deformed. Other times, it may be bent slightly to one side. Although the facial bones on both sides of the child may be abnormal, they may not be as severely deformed. Because of the smaller size of the head, they may not be as noticeable as in other cases of microcephaly.
Microcephaly and primordial dwarfism have similar characteristics, but treatment of both conditions is entirely different. Treatment of both conditions includes surgical intervention, although microcephaly is usually corrected through correction of its bones. Treatment of primordial dwarfism is generally the same as that of microcephaly, but it requires adjustment of the body's structure. Because of this, the patient may also receive anesthetic or steroid injection to reduce the pain associated with mopd2.